INTERVIEW: The American Heart Association on cardiovascular disease care

As part of US Heart Month this February, Hospitals & Healthcare spoke with Dr Mariell Jessup, Chief Science and Medical Officer of the American Heart Association, to find out about the provision of cardiovascular services in the US, and to learn a little more about how assistance providers should adapt their own offerings
Introduction to Dr Jessup:
Dr Jessup is responsible for leading the American Heart Association's (AHA) science enterprise, including the AHA’s science and medical strategy and key strategic science relationships.
An internationally renowned thought leader in heart failure research, prevention and treatment, Dr Jessup’s efforts resulted in heart failure and transplant cardiology becoming a certified secondary subspecialty in 2004. Her tireless and compassionate work as a physician, scientist and mentor have touched the lives of many patients and their families, and young professionals, over her distinguished clinical career.
During her over 24 years of volunteer service to the Association, Dr Jessup has served in many notable roles, including as Chair of the ACC/AHA Heart Failure guidelines in 2009, and the Association’s Committee on Scientific Sessions Program in 2009 and 2010. She was the 2013-14 President of the Association and received its highest honour, the Gold Heart Award, in June 2018.
Hi Mariell, thanks for taking the time to answer some questions. First of all, could you tell us a little about the organisation. When was it first established and what are its key aims?
The AHA was founded in 1924 by six cardiologists as a professional society for doctors. They believed that scientific research could lead the way to better treatment, prevention and, ultimately, a cure for heart disease. At the time of the AHA’s formation, Dr Paul Dudley White, one of the founders, said there was an ‘almost unbelievable ignorance’ about heart disease.
The mission of the AHA is to be a relentless force for a world of longer, healthier lives through research, education and programmes. Since its founding, the AHA has grown into the nation’s oldest and largest voluntary organisation dedicated to fighting heart disease and stroke. A shared focus on cardiovascular health unites more than 40 million volunteers and supporters, as well as more than 2,800 employees.
The World Health Organization notes that cardiovascular diseases are the number one cause of death globally, with one-third of these deaths occurring prematurely in people under the age of 70. What would you say are some of the main contributors to cardiovascular diseases, and how can they be prevented?
The major non-controllable risk factors for cardiovascular disease include increasing age and a family history of heart disease. Controllable factors include: smoking, high cholesterol, high blood pressure, lack of physical activity, obesity, diabetes, stress, excessive alcohol use and poor diet/nutrition.
Fortunately, the controllable risk factors can be prevented through lifestyle changes such as:
- Eating a healthy diet
- Being physically active
- Maintaining a healthy weight
- Living tobacco-free
If individuals have conditions like high blood pressure, diabetes and high cholesterol, they can prevent cardiovascular disease by making the above-mentioned lifestyle changes and managing their condition, as well as taking their medication and working with their healthcare professional on a prevention plan.
What would you say are some of the key ways that assistance providers can adapt their offerings to support members managing chronic heart conditions?
The virtual healthcare visit has been the mainstay of cardiovascular care throughout the pandemic, and will probably be an important component going forward
Most individuals need help with lifestyle improvement. This includes information about safe physical activity regimens, a guide to maintenance of a healthy weight, nutritional information, smoking cessation programmes, blood pressure control, etc. Members with chronic heart conditions need more information about their medications: what they do and why they must be taken. They need to be reminded of warning signposts for their disease, such as undue weight gain, which might indicate fluid retention, or difficulty sleeping. Basic information about prevention and regular reminders for routine vaccinations are also always needed.
Has Covid-19 had an impact on cardiovascular care?
People with heart and stroke symptoms are concerned about going to the hospital. The AHA has been consistent in our message to the US public: absolutely call 911 at the first signs or symptoms of a heart attack or stroke. Doing this quickly can save your life. It’s still the right thing to do, even in this unprecedented time.

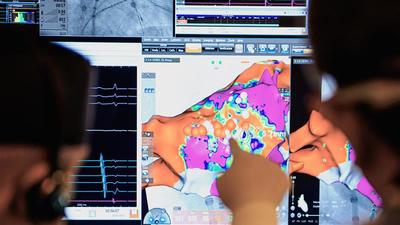
Do you think that technology will play a large role in the management of heart conditions going forward?
Absolutely – we’re already seeing new technologies that are helping people manage heart conditions. From the development of wireless pacemakers to heart tissue bioprinting and using artificial intelligence to predict heart disease in patients. In addition, the virtual healthcare visit has been the mainstay of cardiovascular care throughout the pandemic, and will probably be an important component going forward.

How do you think that both hospitals and assistance providers can wield technology to provide the best services (both preventive and supportive) to their members?
There needs to be a deep dive into which cardiovascular visits can be done safely and effectively on a remote basis, and which visits, and patients, need to be undertaken in an office setting. Are there other models for testing such as EKGs or echocardiograms that can save money and be more time efficient for patients? The healthcare community at large needs to understand what technology for remote visits worked well, what were the deficits, and what needs to be improved. What are we going to do for people with inadequate internet access? What did the healthcare professionals who delivered this remote care think? There needs to be a significant examination of what happened during the pandemic and what we learnt. ■
The American Heart Association on certification standards:
The AHA also offers a number of certifications for US healthcare facilities, one of which is the Advanced Certification in Heart Failure, offered in partnership with the Joint Commission. Could you tell us a little about how the organisation came to offer these accreditations and how it identifies facilities that meet its standards?
The Advanced Certification in Heart Failure is designed to recognise inpatient or outpatient programmes that demonstrate exceptional care and optimise quality of life. Organisations must participate in the GWTG-HF quality improvement programme and follow standardised performance measures. The certification is for an inpatient programme, but is coupled with an assessment of co-ordinated care, including transition to outpatient care providers. It is offered to facilities in the US that meet the criteria for patient load, as well as use evidence-based practices and performance measurements.

February 2021
Issue
In this issue, an interview with the American Heart Association explores how payers and providers can adapt their offerings to help support members with cardiovascular diseases; a feature looking at global healthcare premiums considers the many factors contributing to the rising global cost of healthcare; and we have two industry voices - one from Maxis Global Benefit Network, assessing the implications an ageing workforce can have on IPMI healthcare costs, and another from Swiss Re, underlining the important role that lifestyle data can play in personalising the insurance industry.
Editorial Team
The Editorial Team updates the ITIJ website daily, and works on features for the print edition. With expert industry knowledge and years of experience in writing about complex travel insurance issues, the Editorial Team is ready to investigate and report on the topics that matter most to ITIJ's readers.










February 2025
Issue
Offering readers a deep dive into the issues facing providers and payers of healthcare services around the world. Cost containment, international patient department development, the role of AI in healthcare delivery and more.







