International healthcare and technology – what’s next?

What are the next steps after telehealth, telemedicine, and AI? How far can technology go? Tatum Anderson speaks to experts for their insights
Check any list of trends for the future of healthcare technologies, and artificial intelligence (AI), robotic surgery, wearable technologies, and telehealth appear, alongside 3D-printed organs, biologics, personalised medicine and many others. Their development is driven by changing demographics, lingering Covid-19 affects, widespread labour shortages and escalating costs. Indeed, these evolving technologies present a tantalising solution to many problems, which is why experts at some of the world’s best hospitals helped ITIJ pin down how they might aid health travellers in the coming years.
Future tech
AI is perhaps the most giddying of the innovations, uniting many other technologies. Professor Nima Heidari, expert orthopaedic and trauma surgeon at The London Clinic, who also helps to run a firm that looks into future tech, explained: “AI is essentially a mechanism by which we try and predict something in the future or we try and find things that we may not have been able to find.”
Discriminative AI (rather than generative AI, into which category ChatGPT falls) is able to find patterns in mind-blowingly large amounts of data. Picture the data available in scans and the possible combinations of variables within it, from age to sex, genetic data, heart and blood characteristics. By analysing this
data correlated with the patients’ treatment regimens, AI is able to determine which variables affect treatment outcomes. Once it can see the patterns in the data, researchers can create clever sensors that predict certain outcomes and more. Take AI on retinal scans: “They realised that they could predict how well your diabetes control was, whether you’re about to have renal failure or not,” Professor Heidari said. “Then they realised they could predict whether you’re male or female.”
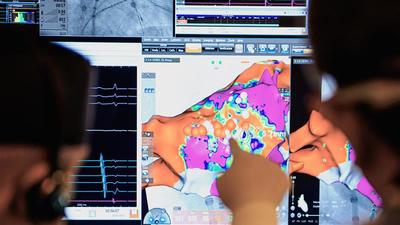
The data AI requires is coming in ever-increasing volumes, from hospital devices to wearable tech (almost too much information to make sense of, say some commentators). In surgery, for example, powerful cameras can be suspended from above the operating theatre. “These allow you to zoom and it replaces incredibly expensive microscopes,” said Professor Heidari. Operators can then wear, say, virtual reality glasses, which magnifies images enormously. “Then you can start processing the images that are being generated,” he said.
Using deep learning and neural networks, the AI system can be educated in screening colonoscopies. Ordinarily the operator is faced with many questions. “Are you seeing abnormal lesions? Should you biopsy or not?” Professor Heidari explained. “If it’s the 10th colonoscopy of the day, the human operator may not be quite as fresh as the first colonoscopy.” This is where AI, which has analysed many thousands of colonoscopies and the outcomes of certain decisions, can assist the doctor with decision-making. “Because the machine doesn’t get tired, it continues to analyse the images and draws your attention to where you need to apply your clinical knowledge to,” he added.
But most important, said Professor Heidari, is AI’s ability to find correlations in the data that even experts in the field cannot imagine. Future applications, therefore, are impossible to predict. “So, for example, from electrocardiograms (ECGs), you might be able to tell the strain on one or the other side of the heart, much more so than a cardiologist ever could,” he added.
Helping patients
AI predictive tools are being developed all the time. Telemedicine specialist Teladoc Health is even using AI’s predictive modelling capabilities to help patients with type 2 diabetes control their blood sugar within a diabetes management programme. “Teladoc Health has a long-standing history of successfully using data to improve health outcomes for our members, and new applications of AI are helping us accelerate our impact,” said Sal Shafiq, Chief Data and Analytics Officer at Teladoc Health, in a statement. “Our ability to use data to empower members in the moment is crucial, but the true power lies in our ability to predict health risks and make prevention a reality.”
Discriminative AI (rather than generative AI, into which category ChatGPT falls) is able to find patterns from mind-blowingly large amounts of data
Similarly, Singapore General Hospital (SGH) created a Combined Assessment of Risk Encountered in Surgery-Machine Learning (CARES-ML) AI tool to predict risk for patients scheduled for surgery. Patients are usually assessed by an anaesthesiologist and surgeon about 10 days before surgery to determine the appropriate level of perioperative care, if they have conditions that might complicate surgery (patients with anaemia, for example, have an increased risk of complications, including infection, stroke or kidney injury), or even if surgery should be postponed.
CARES-ML works by extracting a patient’s medical history, physical status classification, and investigative test results such as X-rays and blood tests from the hospital system to generate a surgery risk report and a score. The higher the score, the higher the risk of an adverse outcome after surgery, explained Geoffrey Gui, Director of the Future Health System at SGH.
“This ultimately improves patient outcomes and enhances patient safety,” he said. So promising is the tech that SGH is considering how the model might also predict other outcomes such as length of hospital stay, and risk of pneumonia and stroke. It is also working with partners to use AI to predict, at diagnosis, which patients with chronic myeloid leukaemia will not respond to conventional treatment. “This means patients could in future receive the appropriate treatment early without delay,” said Gui.
Cost-saving efficiencies
AI is likely to be used by hospitals to make efficiency savings by analysing, say, the flow of patients in the hospital, predicting length of stay, discharge times, optimising the use of the operating theatres and the way to organise staff. Interestingly, generative AI, such as ChatGPT, has been used to save more than 2,800 hours in clinical hours in the eight months to April 2024 by SGH. The hospital has automated the collection, calculation, and dissemination of patient-reported outcome measures (PROMs) filled out by patients for physiotherapists using AI.
Of course, the financial incentives for looking into certain patterns of data may not necessarily be correlated with health outcomes. The danger is that AI is used to deny people health treatments. Insurance companies, for example, may collect data from wearables, such as how many steps are taken in a day, and change premiums based on patterns they find in the data. “They may work out from these that you’re smoking and then say, ‘I’m afraid we’re not going to cover you for lung conditions,’” said one spokesperson.


The robots are here
Another technology predicted to come into its own is robot-based surgery. Earlier this year, the Private Healthcare Information Network (PHIN) said robot-assisted surgeries are already popular. They rose by 928% between 2016 and 2022 in the UK independent sector alone. Robot-assisted procedures mean that fewer open surgeries are necessary. Rather, minimally invasive techniques mean small incisions can be made. Robot-assisted laparoscopic surgery, a minimally invasive surgical technique for complex urological surgery, has been used at SGH for radical prostatectomy (prostate gland removal) and nephrectomy (partial kidney removal), among others.
Our ability to use data to empower members in the moment is crucial, but the true power lies in our ability to predict health risks and make prevention a reality
Gui said that this allows more complex surgery, faster recovery from smaller incision wounds, less pain, lower blood loss and reduced need for transfusion, as well as better vision and tissue dissection from a magnified view and use of special robotic instruments.
However, though robots are already extremely sophisticated technologies, there are currently limitations, said Dr Mohamad Bydon, a neurosurgeon who specialises in complex spinal surgery and spinal oncology at the US Mayo Clinic. He currently performs minimally invasive procedures on the spine, aided by robots that insert what he terms “instrumentation”, such as pedicle screws, into the vertebral bodies or bones. “Robotic surgery
allows us to be very accurate, down to the millimetre, in terms of accuracy of placement of that instrumentation, and therefore reduces the rate of replacement or misplacement of instrumentation,” he said. While robots today place screws into the spine, in future they may remove bone to free up compression on nerves. The next steps will be even more minimally invasive approaches and smaller and smaller incisions.
Importantly, robots today perform only part of the surgery. Dr Bydon believes that, over time, as the robotic guidance improves, they may be able to perform more and more phases of the procedure. “I would emphasise, you always need a surgeon in the room,” he said. “There is no remote surgery done.”
Of course, remote robotic surgery has been talked about for years, and is even trialled in other specialties. But as a routine tech in, for example, spinal operations, it still has a long way to go. “The technology is getting closer and closer. So it’s just a matter of time,” said Dr Bydon.
The potential for joint surgeries is great, then. “Picture the scenario where one operator is doing surgery in the United Kingdom, and they could be jointly doing it potentially with a surgeon, say, in the United States,” he said. “As long as there’s access to the software, and one of the surgeons is there, then potentially those surgeries could be done jointly.”
The future of telemedicine
This is where telemedicine linked to robotic surgery would be vital. Gui agreed that, in future, remote surgery would be done through telementoring. That would mean medical training and education would not be limited by distance. “It can foster interprofessional collaborative learning among the global medical community and provide access to specialised care, especially to underserved areas,” he added.
Of course, the use of telemedicine exploded during the pandemic, and the ability to communicate with audio and visual input is in place and mature, according to Gui.
“However, there are still limits to completely replacing or replicating the in-person medical consultation,” he said. What does not exist yet is a single seamless user portal for both patients and healthcare providers, integration of patient-provided data into electronic health records and ambient in-home monitoring.
If imaging, point-of-care testing, and other investigations that are typically done in a hospital can be done elsewhere, it will significantly increase the range of patients who can be managed remotely and in the comfort of their homes.
“Healthcare providers may be able to see their patients’ blood glucose or vital signs trends using dashboards embedded in the electronic health record, discuss the readings with them during teleconsultation sessions, and make timely medication adjustments,” Gui explained.
Wearable devices will be crucial in moving towards that hospital-at-home scenario in the future. Certainly the devices have come a long way and can help with endocrinology (blood glucose level monitoring) and cardiovascular (telemetry for cardiac rhythms, blood pressure measurement). This is important given the rate at which conditions such as diabetes are rising across the world.
Remote monitoring will be vital, say experts. Future wearables, much like virtual reality (VR), surgery and AI, however, will have to overcome the range of challenges they face today. Wearables are not always of clinical grade, and there are high attrition rates and adoption barriers, said Gui.
Professor Heidari added that the accuracy of the information recorded can also be variable (pulse oximetry can be adversely affected by skin colour, for example). “You can see how some of these technologies will have difficulties in picking up accurate information,” he said. “But that is a problem which is being solved.”

November 2024
Issue
This month we look at affinity partnerships and ask if online travel agencies are the perfect partners for insurers; we cover the trends around cruising in the Mediterranean; we delve into the specifics of the Austrian healthcare system; plus we examine international healthcare and technology, asking how far can technology go.
Tatum Anderson
Tatum Anderson is a journalist and has written in-depth features for ITIJ and its supplements for over 12 years. An experienced tech, business and global health specialist, she specialises in writing about all manner of medical travel and technology, from AI and telemedicine to crew health and cost containment. She routinely interviews high-level executives from international hospitals and insurers to assistance companies and air ambulance firms worldwide. Tatum has also written for a range of high-profile publications including The Bulletin of the World Health Organization, BBC News Online and The Guardian. She was a stringer for The Economist and has contributed to The Lancet, BMJ and Nature.










February 2025
Issue
Offering readers a deep dive into the issues facing providers and payers of healthcare services around the world. Cost containment, international patient department development, the role of AI in healthcare delivery and more.







