The magic of telemedicine

Telemedicine is fast becoming the new normal. However, there are barriers to its implementation. Could insurance companies help build traction? Tatum Anderson investigates
Patients who need to see a doctor but can’t manage a face-to-face appointment are doing so via their PCs or mobile phones. They are prepared to consult on all sorts of complaints too. From cardiology to dermatology, gynaecology and even psychiatry and pathology, there are emerging telemedicine services.
Expatriates are using virtual healthcare services provided by physicians located at home, and home-based citizens are seeking less expensive care via telemedicine from healthcare providers located abroad. Doctors are even using telemedicine to talk to other doctors, as is the case at US hospital Cedars-Sinai Medical Center.
With 350 million smartphone users in India, many of whom live far from health services, telemedicine has found a natural space. Jithu Jose, Head of International Business Division of the Apollo Middle East Consultancy, UAE, said: “Our telehealth service is one of the largest such service in Asia and we cover some 30 countries on it.” Patients can book appointments, have online consultations and health checks, and there are online health records and homecare services too.
A doctor can diagnose an ear infection via video chat, but they won’t notice the skin discoloration on a patient’s arm that could be something more serious
Likewise, Pakistan-based DoctHERS matches patients and their families with the vast pool of female doctors who are unable to practise outside the home, for cultural or childcare reasons. The platform is being offered to corporates to plug the massive gap in healthcare services for employees within their supply chains in Pakistan, according to Asher Hasan CEO of DoctHERS. So prevalent is telemedicine, that research firm Mordor Intelligence estimates the market will grow from $US23.2 million in 2015 to a massive $66.6 million by 2021.
And, the world’s largest insurance companies are offering telemedicine services to their customers. Cai Glushak, a Clinical Professor of Medicine and International Medical Director at AXA Partners, which is considered one of the early adopters, said: “In our industry, telemedicine can serve two functions: cost-savings and convenience. Depending on your target client, it will have different attractiveness. Telemedicine really maximises its cost-effectiveness for payers responsible for medical costs. So, this applies to traditional health insurers, certain expat benefit programs and travel insurance that covers medical expenditure,” he explained.
“Beneficiaries will be well-served when it avoids the need to find a doctor, especially in unfamiliar and remote locations. Where access is a problem it is a truly valuable service. In this case, a typical 10- or 15-minute teleconsultation may avoid a costly and protracted emergency room or doctor’s office visit – along with all the potentially unnecessary testing that would follow.”

Worldwide connections
Doctor Care Anywhere provides telemedicine services for some of the world’s biggest insurance companies. The platform enables patients around the world to consult with general practitioners (GPs) for AXA PPP, Nuffield Health and Aon to name a few. So far, the platform has been accessed from 108 different countries in the last 18 months, said Dr Eric Miller, Global Head of Corporate at the company.
When a customer or patient requests an appointment, the doctor service works something like this: the patient is asked to fill in an online form, which asks for pertinent information. That is sent to a doctor’s panel, which decides whether this is an emergency case, or whether to offer a GP appointment via videoconferencing, or if not convenient, by phone. Around 60 per cent of the patients opt for video-conferencing appointments (the others, who prefer a phone consultation, are usually calling from work or are at a location where broadband is limited).
Miller believes insurance companies are offering this service because it saves them money when dealing with both tourists and expatriates who would like access to the level of healthcare that they are used to at home. “Essentially, we are the policyholder’s ‘custodian’ when they need medical attention in a foreign country. In most travel scenarios, an ill patient either goes to the concierge to get the hotel Doctor or to a local doctor,” he said. “This disjointed experience ends up costing two to three times the price of a virtual consult and is all-too-often a scary experience for the patient. We are the safe and familiar ‘first port of call’ for the patient and take over directional care responsibility from the patient’s first contact through to managing that patient’s journey within the insurer’s network.”
There are many flavours of telemedicine. Often called virtual health or virtual doctors, a market of online GP services has flourished over the last five years.
A typical 10- or 15-minute teleconsultation may avoid a costly and protracted emergency room or doctor’s office visit
GPs may work for a number of different platforms, depending on when they are free. Some services provide a 10-minute consultation as standard, and then if patients require longer consults, they pay for extra time. Others do not see children. Some services like his own, said Miller, only take on highly qualified doctors – such as those who are registered with the UK’s General Medical Council, have worked between five and 10 years after graduation, have been trained in telemedicine and commit to a minimum of 15 hours per fortnight to stay on the platform.
He believes that’s vital for maintaining quality. “Our intention was never to be an uber-type provider, where patients are matched with random doctors that have spare time. We wanted to make sure the doctors were ours and our clinical governance meant that patients received the highest quality care wherever in the world they happened to be,” he said.
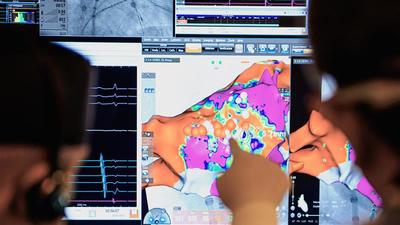
Picking up on patient cues
But are there limitations to the kinds of treatments that can be diagnosed or managed online? Miller says 65 to 75 per cent of GP consultations can be resolved in one sitting. The rest are referrals and repeat appointments (and no emergency cases are taken). He believes it is possible to see to most complaints, given the appropriate training is provided. “A great doctor is able to diagnose based on history, presenting complaint and clinical signs,” he explained. “Our training, for this new technical edge, requires doctors to pick up on subtle patient cues within the videoconference – by what the patient is saying, and how they are saying it. There are nuances doctors must be very sensitive to through video rather than being there in person. It’s more ‘web-side’ manner than ‘bed-side’ manner.”
What with advances in smart phone, video and broadband technologies, telemedicine has come on leaps and bounds. Remote patient monitoring devices and apps that are able to feed data into the services are all helping to improve the use of the technology too. Any restraints in using telemedicine services are now unlikely to be down to the quality of the technology itself, but attitudes to the technology in patients and doctors, experts say.
For example, many of the target populations are still not tech savvy enough and may have difficulty handling a video-interface, which requires proper browser and webcam functionality (many users, especially older patients, prefer a simple telephone conversation). Bandwidth is often a problem in many locations – and not just developing countries. So, transmitting complicated data and video requires bandwidth – may vary at the customer end.
The age of the doctors is relevant too, said Christine Carrillo, CEO and co-Founder of JOANY, a healthcare concierge service that allows consumers to submit online questions about anything from doctor’s appointments to medical bills and what’s covered by their plans – and therefore has a view of the entire healthcare market. “Telemedicine is a costly venture and requires a proper network, infrastructure and training to implement. While newer physicians are often trained to diagnose remotely, it is a skill often lost on physicians who started practising before telemedicine existed or while it was in its infancy,” she said. “It’s a concept all medical providers should consider, but available resources often dissuade implementation.”
Legal issues are a major barrier to the use of telemedicine as well. Some countries and states may actually require videoconferencing as a condition of performing telemedicine, for example (whereas many platforms offer the ability to provide telemedicine via phone as well as videoconferencing).
In addition, some countries ban healthcare providers from providing services unless they hold a valid license or registration in the country or local jurisdiction where they are providing such services.
AXA Partner’s Glushak said issues of licensing have a knock-on effect when it comes to prescriptions. “The challenge is pairing the service with the ability to fill a prescription,” he explained. “Country restrictions may limit the authority of the telemedicine physician to arrange a prescription in the country where the patient is located.”
Many providers get around this by partnering with local doctors to produce prescriptions, or if volume demands it, opening an independent unit within the country. AXA Assistance calls its combination of approaches a prescription solution, where it collaborates within a growing number of countries in combination with providing telemedicine from abroad.
Luckily, gradually the rules are being changed. A European Union (EU) physician registered in one EU country can provide virtual care services to patients in another EU member state, even if that physician is not registered in the member state in which the patient is located. That is part of the EU Cross-Border Healthcare directive.
Ironing out challenges
Some countries have been ahead of the game. Mutual recognition and related rules laws reduce some of the burden – Australia and New Zealand as far back as 1992 created a mutual recognition model permitting physicians in Australia and New Zealand to practise in certain territories in Australia and New Zealand where they are not registered.
Even in the US, over the last few years, there have been efforts to streamline and simplify physician licensing across state lines because so many prevent one doctor from providing services to telemedicine patients who may be located in a different state. Indeed, some states have even begun to enact laws requiring commercial health plans to cover medical services provided via telehealth to the same extent they cover medical services provided in-person.
If a doctor fails to diagnose a serious disease and does not also have a longstanding provider-patient relationship, that could spell trouble
Gallagher Healthcare Practice, a US-based insurance broker and risk management provider, warns of future legal problems, however. If a doctor fails to diagnose a serious disease and does not also have a longstanding provider-patient relationship, that could spell trouble. “That could lead to increased liability losses,” said a report carried out by Gallagher Healthcare Practice, in conjunction with a Washington DC law firm. Such problems may be more prevalent in a number of chronic diseases – such as cardiovascular disease – where without good management, high severity cases have very bad patient outcomes, it reckons. “Coupled with the relative novelty of virtual care, telemedicine related to these conditions may lead to increased liability losses. One thing seems certain, negligible malpractice activity in telehealth is unlikely to continue,” according to the report.
As legal challenges are ironed out, it may be up to organisations like insurance companies to help overcome the reluctance to adopt technology. Insurance companies could do their part to build up traction for such services, said Miller of Doctor Care Anywhere. He reckons that people are starting to renew policies with insurers who offer telemedicine services. He says net promoter scores (NPS), which measure how willing customers are to stay with a service, prove this. “We have consistently scored higher above 85 on our NPS. This is really ‘sticky’ and provides a ‘halo effect’ for our insurance partners ... sometimes raising their NPS by 50 per cent.”
How successful a telemedicine service is depends on whether the insurer wants to be the gatekeeper, and controls the advertising, he said. “If it’s a service that’s just advertised as, ‘Yes, we have telemedicine’, it won’t get used much,” he said. “If we have access to the patient, by email, text or bespoke messaging, there is a much higher utilisation rate.”
But JOANY’s Carrillo says, as convenient as telemedicine is, nothing can replace in-person interactions with doctors. “Sure, a doctor can diagnose an ear infection via video chat, but they won’t notice the skin discoloration on a patient’s arm that could be something more serious,” she said. “A patient can only rely on telemedicine to address the concern at hand, not to proactively identify other areas of concern.”
Telemedicine also relies more heavily on patients to maintain a proper treatment regimen. “Patients can misreport the severity of an issue to avoid a higher medical bill or skirt tough conversations about medical problems,” she concluded.

April 2018
Issue
Tatum Anderson
Tatum Anderson is a journalist and has written in-depth features for ITIJ and its supplements for over 12 years. An experienced tech, business and global health specialist, she specialises in writing about all manner of medical travel and technology, from AI and telemedicine to crew health and cost containment. She routinely interviews high-level executives from international hospitals and insurers to assistance companies and air ambulance firms worldwide. Tatum has also written for a range of high-profile publications including The Bulletin of the World Health Organization, BBC News Online and The Guardian. She was a stringer for The Economist and has contributed to The Lancet, BMJ and Nature.










February 2025
Issue
Offering readers a deep dive into the issues facing providers and payers of healthcare services around the world. Cost containment, international patient department development, the role of AI in healthcare delivery and more.







